Glaucoma - The Complete Guide
All the medical information on early diagnosis, types, essential exams, and advanced treatment and surgical methods

Prof. Ari Leshno
Senior Ophthalmologist, Glaucoma & Cataract Specialist and Head of Innovation & Research
Prof. Ari Leshno is a senior physician in the Glaucoma Service, Clinical Associate Professor of Ophthalmology at Tel Aviv University, and a graduate of the Talpiot Excellence and Leadership Program at Sheba Medical Center. He completed his residency with distinction at the Goldschleger Institute and a glaucoma fellowship at Columbia University, New York. An active researcher with 80+ publications, two patents in medical devices, and recipient of multiple awards for excellence.
What is Glaucoma?
Glaucoma is a group of chronic eye diseases that cause damage and degeneration of the optic nerve, resulting in a decline in visual function. It is one of the leading causes of blindness worldwide and the leading cause of irreversible blindness. Therefore, early detection and appropriate treatment are essential to prevent damage and preserve quality of life.
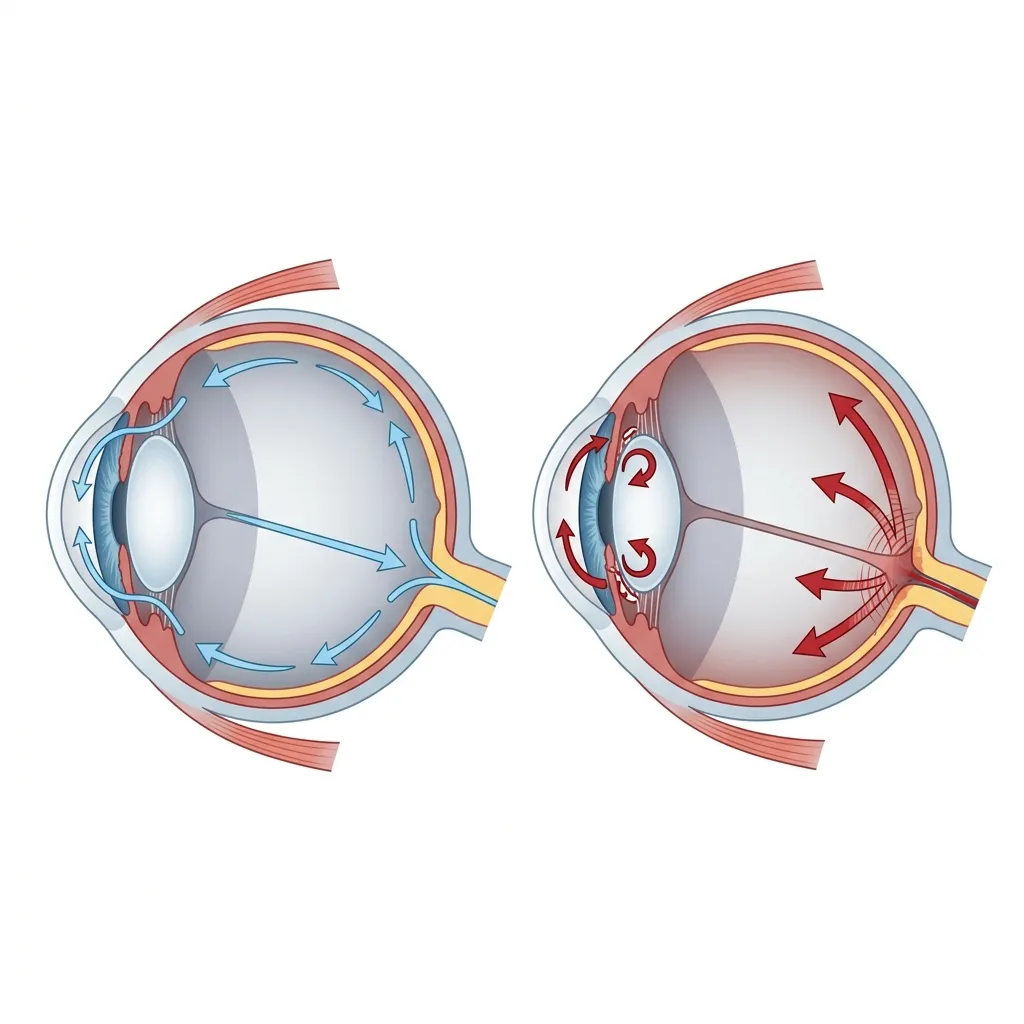
Comparison: Healthy eye drainage (left) vs. blocked drainage, built-up pressure and optic nerve damage in glaucoma (right).
How Does Glaucoma Develop?
Glaucoma results from chronic damage to the nerve fibers that form the optic nerve and the cells from which these fibers originate. The mechanism of destruction is not fully understood but is likely related to a combination of mechanical pressure on the fibers, impaired blood flow to this layer of the retina, and possibly secondary inflammatory processes. In most cases, the changes develop slowly over years and progressively worsen with age.
"The Silent Thief of Sight"
As noted above, the damage caused by glaucoma typically develops gradually and slowly. Naturally, the brain learns to compensate for the deficit (especially when damage begins in only one eye), and patients do not notice the change until relatively late stages when significant damage has already occurred. Additionally, in many cases the damage starts more prominently in the periphery of the visual field, which is less noticeable in daily functioning. Therefore, by the time patients notice vision changes, significant and irreversible damage may have already occurred, earning glaucoma its nickname 'the silent thief of sight.'
Who Is At Risk?
Glaucoma has numerous risk factors including: family history of glaucoma (especially first-degree relatives), ethnicity, high myopia (nearsightedness) or hyperopia (farsightedness), thin corneas, chronic steroid use, history of eye trauma, intraocular inflammation, previous eye surgeries, low blood pressure, and more. Currently, the only treatable risk factor is intraocular pressure, and treatment focuses on lowering intraocular pressure to levels that slow and even halt disease progression. Regular eye exams are critical for early detection, especially if you have one or more risk factors.
Symptoms and Warning Signs
It is important to emphasize that the absence of symptoms or a sensation of vision disturbance does not rule out glaucoma. Furthermore, in most cases, elevated intraocular pressure cannot be felt even when very high. Therefore, routine monitoring that allows tracking of the disease is essential. An attack of acute angle-closure glaucoma is an exceptional case where a sharp rise in intraocular pressure can lead to sudden eye pain, headache, nausea, blurred vision, and halos around lights, which is a medical emergency requiring immediate treatment.
Why Early Detection Matters
Currently, there is no treatment that can repair damage to the optic nerve caused by glaucoma, and vision loss cannot be restored. However, there is a wide range of treatments that help slow the rate of disease progression and even stop it, so the disease can be managed effectively, especially when detected early. Comprehensive eye examinations that include intraocular pressure measurement, optic nerve evaluation with OCT imaging, and visual field testing are the best defense against vision loss. Prof. Leshno recommends baseline screening starting at age 40, with more frequent exams based on risk factors. In cases of strong family history or early onset, genetic testing should also be considered.
Types of Glaucoma
There are several types of glaucoma, each with distinct characteristics and treatment approaches. Understanding the specific type is essential for effective management.

Visual field simulation: Normal wide-angle vision (left) vs. advanced peripheral vision loss (tunnel vision) typical of glaucoma (right).
Open-Angle Glaucoma
The most common form, accounting for about 90% of all cases. The drainage angle remains open, but the trabecular meshwork becomes less efficient over time. Pressure builds gradually, and vision loss happens slowly over years. It typically affects both eyes, though often unevenly. Treatment usually begins with medicated eye drops and may progress to laser therapy or surgery.
Angle-Closure Glaucoma
Occurs when the iris bulges forward and physically blocks the drainage angle. Can develop gradually (chronic) or suddenly (acute). Acute angle-closure is a medical emergency causing sudden severe eye pain, headache, nausea, and blurred vision. Risk factors include farsightedness, small eyes, and East Asian heritage. Treatment typically involves laser iridotomy to create a new drainage pathway.
Normal-Tension Glaucoma
In this form, optic nerve damage occurs even though intraocular pressure remains within the statistically normal range (below 21 mmHg). This suggests that some optic nerves are more vulnerable to pressure damage, or that other factors such as blood flow to the optic nerve play a role. Treatment aims to lower pressure further below the patient's baseline.
Secondary and Congenital Glaucoma
Secondary glaucoma results from other eye conditions, medications (particularly corticosteroids), injuries, or systemic diseases. Pseudoexfoliation glaucoma and pigmentary glaucoma are common subtypes. Congenital glaucoma is present at birth due to abnormal drainage angle development and typically presents in infancy with tearing, light sensitivity, and cloudy corneas.
Glaucoma Evaluation & Diagnostic Exams
Diagnosing and monitoring glaucoma relies on a combination of clinical examinations and advanced instruments. Each test provides unique information about the condition of the eye, and together they enable the physician to obtain a complete and accurate picture of the disease and to customize treatment on an individual basis.
OCT Scan
Optical Coherence Tomography (OCT) is a non-invasive imaging technology that uses light waves to capture high-resolution cross-sectional images of the retina and optic nerve. It is an essential tool in diagnosing and monitoring glaucoma.
OCT uses near-infrared light to create detailed cross-sectional images of the retinal layers, similar to how ultrasound uses sound waves. The scan is quick, painless, and non-contact (it takes only a few seconds per eye). The technology can measure the thickness of the retinal nerve fiber layer (RNFL) and the ganglion cell layer with micrometer precision.
In glaucoma care, OCT is used to measure the thickness of the retinal nerve fiber layer around the optic nerve head and the ganglion cell-inner plexiform layer in the macula. Thinning of these layers indicates damage from glaucoma, often before any vision loss is noticed by the patient. OCT can detect structural damage years before functional changes appear on visual field tests.
Serial OCT scans taken over time allow your doctor to track disease progression precisely. Modern OCT software includes progression analysis tools that can detect small changes in nerve fiber thickness, helping to determine if treatment is effectively controlling the disease. Prof. Leshno uses the latest OCT technology to provide the most accurate and detailed imaging available.
The OCT exam is quick and comfortable. You will sit in front of the machine and look at a target light while the scan is performed. No drops or contact with the eye is required for most OCT scans. The entire process takes about 5–10 minutes for both eyes. Results are available immediately and will be reviewed with you during your appointment.
Visual Field Test
What is a Computerized Visual Field Test?
A standard automated perimetry (SAP) test measures the retina's sensitivity threshold to light at various points. By comparing your personal results to data of healthy individuals of the same age, it helps identify areas of abnormally decreased sensitivity (scotomas).
The test is performed sitting in front of a dome-shaped instrument. One eye is covered, and with the other eye, you look at a central fixation target. Throughout the test, flashes of light of varying intensities will appear in different locations in your visual field. Every time you notice the light - even if it is very faint - you press a hand-held button to indicate that you detected the stimulus.
Many tend to think that if they can read the small letters at the optometrist (visual acuity), their vision is entirely normal. In reality, the situation is more complex. Visual function comprises many components beyond visual acuity, such as color vision, visual field, contrast sensitivity, spatial vision, and 3D vision. In the early stages of glaucoma, functional damage tends to be localized and may predominantly affect the peripheral visual field, practically having no effect on a visual acuity test.
The brain and eyes' compensatory mechanisms are the reason it's hard to notice the damage. This is a tremendous but simultaneously cruel ability. The brain knows how to "fill in" the missing information by combining data from the healthy areas and the other eye. Because the damage progresses gradually, the brain learns to compensate for "holes" in the visual field so that it interferes less with daily life. While this amazing ability helps cope with the damage, it also prevents the patient from realizing there's a problem, and often patients only start to "feel" the glaucoma when there's significant irreversible damage.
There are several testing devices, and each can be configured with different tests depending on field size, testing strategy, stimulus size, and more. The most common test today is the "24-2" which tests the central and intermediate visual field. Since the resolution of this test is not always high enough to detect central damage, a "10-2" test focusing on the 10 central degrees of vision is often performed in parallel or alternately.
Absolutely. For reliable glaucoma monitoring, it is best to perform the test on the same type of device and under the same conditions. Using different machines or software versions can create "noise" that makes it harder to identify changes. Performing the test on the same machine allows the creation of a trend analysis graph that helps evaluate and identify long-term changes.
This is not a "pass/fail" test: Don't try to "guess" where the light will appear.
Concentration and rest: The test requires focus. If you feel tired, you can pause for a moment to rest.
Optical correction: The test is performed with near-vision corrective lenses (if needed) to ensure the result reflects the optic nerve's condition, not a refractive error.
Testing each eye typically takes a few minutes. Together with preparation, the whole process takes about 20-30 minutes. Note that the duration is also affected by the type of field and strategy used, and lack of cooperation can prolong the test.
Interpreting the test is a task for a glaucoma specialist. The printout includes complex statistical indices (like MD and PSD) and probability maps. A normal test is one where the sensitivity at all points is within the normal range for your age, but we always need to consider stability compared to past tests.
Intraocular Pressure (IOP)
Intraocular pressure (IOP) is the fluid pressure inside the eye. It is a key factor in glaucoma development and the primary target of treatment. Understanding IOP is essential for every glaucoma patient.
Normal IOP typically ranges from 10 to 21 mmHg, though what is 'normal' varies between individuals. Some people develop glaucoma damage at pressures below 21 mmHg (normal-tension glaucoma), while others tolerate pressures above 21 mmHg without damage (ocular hypertension). The goal of treatment is to reach a 'target pressure' that prevents further optic nerve damage for each individual patient.
The gold standard for IOP measurement is Goldmann applanation tonometry, performed during a slit lamp exam with anesthetic eye drops. Non-contact tonometry (the 'air puff' test) is also commonly used for screening. Newer methods include rebound tonometry (iCare), which requires no drops. IOP can fluctuate throughout the day, so your doctor may recommend measurements at different times.
IOP naturally fluctuates during the day, typically being highest in the early morning. Factors that can elevate IOP include certain body positions (lying flat), tight neckwear, straining (Valsalva maneuver), caffeine intake, and certain medications (corticosteroids). Corneal thickness also affects IOP readings, as thicker corneas may overestimate pressure, while thinner corneas may underestimate it.
The primary goal of glaucoma treatment is to lower IOP to a level that prevents further optic nerve damage. Studies have shown that reducing IOP by 20–30% from baseline significantly reduces the risk of progression. Treatment options include eye drops, laser therapy, and surgery. Prof. Leshno will determine your target pressure based on your specific type of glaucoma, severity of damage, life expectancy, and risk factors.
Corneal Thickness (Pachymetry)
What is the Cornea?
The cornea is the clear window at the front of the eye. Its main function is to bend incoming light rays and focus them on the retina, while simultaneously serving as an outer protective layer. Just as people differ in height or eye color, there is natural variation in corneal thickness from person to person.
How does corneal thickness relate to glaucoma and intraocular pressure?
Evaluating intraocular pressure (IOP) is largely based on applying gentle physical force to the surface of the cornea, and instruments are calibrated according to average corneal thickness. When the cornea is thinner than average, measurement devices may show a pressure lower than it truly is. Conversely, when the cornea is thicker than average, the device may show an artificially high pressure.
Currently, there is no precise calibration formula to correct pressure measurement based on corneal thickness. However, corneal thickness must be taken into account during every intraocular pressure measurement to more accurately assess the condition of the eye.
Beyond its effect on technical measurement, large-scale medical studies have proven that a thin cornea is an independent risk factor for the development and progression of glaucoma, regardless of the measured pressure level. Conversely, a thick cornea serves as a protective factor against the development of glaucoma. Therefore, knowing your corneal thickness is essential for building a complete risk profile.
In most cases, corneal thickness does not change significantly after adolescence. However, eye surgeries, especially laser vision correction surgeries, can affect the structure of the cornea. These surgeries act by reshaping and thinning the cornea. A patient who underwent laser vision correction in the past will have a thinner cornea, which requires special consideration when evaluating intraocular pressure years later. Various eye diseases can also cause thinning (keratoconus) or thickening (corneal edema), so a thorough history is critically important.
Corneal thickness is measured non-invasively and involves no pain or discomfort. There are a variety of instruments used to evaluate corneal thickness. The measurement can be done using several technologies:
- Ultrasound Pachymetry: The use of sound waves for a highly accurate, point-specific evaluation of corneal thickness.
- Optical Pachymetry: The use of light rays for non-contact mapping of corneal thickness at microscopic resolution.
Additional Diagnostic Tests
Intraocular Pressure Measurement (Tonometry)
Intraocular pressure measurement is one of the most fundamental tests in glaucoma evaluation. The gold standard is Goldmann applanation tonometry, performed at the slit lamp after local anesthetic drops. Additional methods include rebound tonometry (iCare), which does not require drops, and non-contact tonometry ('air puff') for initial screening. Intraocular pressure varies throughout the day, so repeated measurements at different times may be necessary.
Corneal Thickness (Pachymetry)
Measuring corneal thickness is important because it affects the accuracy of intraocular pressure measurement. Thick corneas may cause overestimation of pressure, while thin corneas may lead to underestimation, potentially causing delayed diagnosis. Thin corneas are also considered an independent risk factor for glaucoma. The test is performed using an ultrasound or optical device, and is quick and painless.
Visual Field Testing (Perimetry)
Visual field testing measures visual function across different areas of the visual field. It is a critical test that reveals the functional impact of glaucoma (areas where light sensitivity has been impaired). The test is performed using a computerized device (Humphrey) that identifies defects characteristic of glaucoma. Results over time allow monitoring of disease stability or progression.
Gonioscopy
Gonioscopy allows the physician to look directly at the drainage angle of the eye, the structure through which intraocular fluid drains. The examination is performed using a special lens placed on the eye. It is essential for classifying the type of glaucoma (open-angle vs. angle-closure), identifying pathological findings in the angle, and planning treatment. The test is quick and generally does not cause significant discomfort.
Fundus Photography
Color photography of the fundus objectively documents the appearance of the optic nerve. The photographs allow the physician to compare the nerve's condition over time and identify gradual changes. Important findings include cup-to-disc ratio, presence of small hemorrhages, nerve tissue thinning, and blood vessel patterns. Photography complements the OCT exam and enables direct visual assessment.
Slit Lamp Examination
The slit lamp is a specialized microscope that allows the physician to examine all eye structures under magnification. In the context of glaucoma, the examination enables evaluation of the anterior chamber, chamber depth, iris condition, lens, and angle. Combined with special lenses, the optic nerve and retina can also be examined. This is the foundational examination of every eye visit and provides critical information for diagnosis and follow-up.
Biometry
Biometry is a precise measurement of eye structures, including eye length, anterior chamber depth, and lens thickness. In the context of glaucoma, these measurements are important for identifying short eyes at risk for angle-closure glaucoma. Biometry is also essential for planning cataract surgery in glaucoma patients, where choosing the appropriate lens can affect intraocular pressure.
Genetic Testing
In recent years, significant progress has been made in understanding the genetic factors behind glaucoma. Genetic testing is especially recommended in cases of strong family history, early-onset glaucoma, or unique forms of glaucoma. Identifying specific genetic mutations (such as MYOC, OPTN, and others) can aid in early diagnosis of at-risk family members and sometimes also influence treatment selection. Prof. Leshno incorporates genetic testing as part of a comprehensive evaluation when relevant.
Glaucoma Treatment & Surgeries
Lowering intraocular pressure is the cornerstone of glaucoma management. Multiple treatment approaches are available, and the best strategy is tailored to each patient's specific needs and disease characteristics.
SLT Laser Treatment Diagram
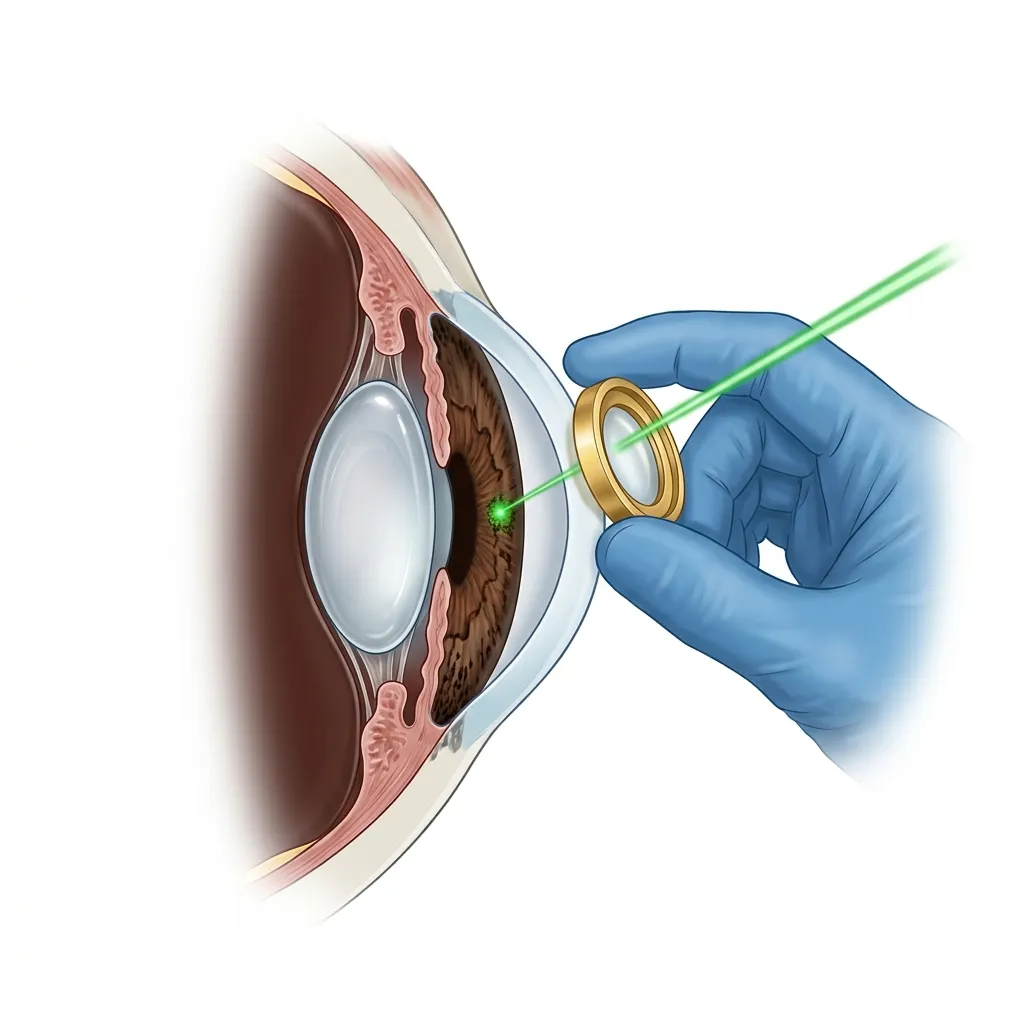
- Goniolens: Special lens placed on the cornea to direct the laser beam.
- Laser Beam: Focused green laser targeting the drainage tissue.
- Drainage Angle: Trabecular meshwork (TM) where fluid outflow is restored.
SLT laser treatment: A focused laser beam stimulates the drainage angle (trabecular meshwork) to restore normal fluid outflow.
Medical Treatment (Eye Drops)
Eye drops are the most common initial treatment for glaucoma. Proper use and adherence to your drop regimen are essential for effective pressure control and preventing vision loss.
Types of Glaucoma Eye Drops
Prostaglandin analogs (Latanoprost, Travoprost, Tafluprost) are the most commonly prescribed first-line drops (used once daily at bedtime, they increase fluid outflow and can lower IOP by 25–35%). Beta-blockers (Timolol) reduce fluid production and are used once or twice daily. Alpha-agonists (Brimonidine) and carbonic anhydrase inhibitors (Dorzolamide, Brinzolamide) provide additional pressure reduction through different mechanisms.
Combination Drops
When multiple medications are needed, combination drops that contain two active ingredients in a single bottle can simplify your regimen. Common combinations include Timolol-Dorzolamide, Timolol-Brimonidine, and Timolol-Latanoprost. Using combination drops reduces the total number of bottles and daily instillations, which improves adherence and reduces preservative exposure.
Proper Drop Technique
Correct instillation technique ensures the medication reaches the eye effectively. Tilt your head back, pull down the lower eyelid to create a pocket, and instill one drop. Close your eye gently (don't squeeze) and press on the inner corner of the eye (punctal occlusion) for 1–2 minutes. This reduces systemic absorption and minimizes side effects. Wait at least 5 minutes between different drops.
Laser Treatments (SLT, LPI)
Laser treatments offer effective, minimally invasive options for managing glaucoma. These procedures can reduce dependence on eye drops and are performed in an office setting with minimal downtime.
Selective Laser Trabeculoplasty (SLT)
SLT is the most commonly performed glaucoma laser procedure. It uses short pulses of low-energy laser light to stimulate the trabecular meshwork, improving natural drainage. Success rates range from 70-80%, achieving IOP reduction of 20-30%. The procedure takes about 5 minutes, is nearly painless, and can be repeated if the effect diminishes over time. Recent studies (LiGHT trial) support SLT as an effective first-line treatment.
Laser Peripheral Iridotomy (LPI)
LPI is the primary treatment for narrow-angle and angle-closure glaucoma. A small hole is created in the peripheral iris using a YAG laser, allowing fluid to flow freely between the anterior and posterior chambers. This relieves pupillary block and opens the drainage angle. The procedure is quick, performed in the office, and is both a treatment and a preventive measure for the at-risk fellow eye.
Cyclophotocoagulation
This laser procedure targets the ciliary body, the tissue that produces aqueous fluid, to reduce fluid production and lower IOP. Transscleral cyclophotocoagulation (TCP) and endocyclophotocoagulation (ECP) are available options. Micropulse cyclophotocoagulation is a newer, gentler approach with fewer side effects. These procedures are typically reserved for more advanced or refractory cases of glaucoma.
Glaucoma Surgeries (MIGS & Traditional)
When medications and laser treatments are insufficient to control intraocular pressure, surgical intervention may be necessary. Modern glaucoma surgery offers a range of options from minimally invasive procedures to traditional filtration surgery.
Minimally Invasive Glaucoma Surgery (MIGS)
MIGS represents a paradigm shift in glaucoma surgery, offering safer alternatives with faster recovery. These procedures include trabecular micro-bypass stents (iStent), Schlemm's canal procedures (canaloplasty, OMNI), and subconjunctival drainage devices (Xen gel stent). MIGS are especially suitable for mild to moderate glaucoma and can often be combined with cataract surgery. Prof. Leshno has extensive experience with the full range of MIGS procedures.
Trabeculectomy
Trabeculectomy remains the gold standard of glaucoma filtration surgery for significant IOP reduction. A small flap is created in the sclera to allow controlled outflow of fluid from the eye into a filtering bleb under the conjunctiva. With proper management including antimetabolites (Mitomycin C), trabeculectomy can achieve excellent long-term pressure control. Prof. Leshno trained in advanced trabeculectomy techniques at Columbia University.
Glaucoma Drainage Devices
Tube shunt surgeries (Ahmed valve, Baerveldt implant) involve placing a small tube in the eye connected to a plate on the external surface of the eye. Fluid drains through the tube to the plate, where it is absorbed by surrounding tissues. These devices are particularly effective for complex or refractory cases, neovascular glaucoma, and eyes with previous failed filtration surgery.
Recovery and Follow-Up
Glaucoma surgery recovery time varies by procedure type. MIGS procedures typically allow return to normal activities within days. Trabeculectomy and tube shunt surgeries require more careful postoperative management over several weeks, including frequent follow-up visits and medications. Activity restrictions during recovery may include avoiding heavy lifting and strenuous exercise. Prof. Leshno will guide you through every step of your recovery.